 企业邮箱
企业邮箱






3. Discussion of the Future of Regenerative Medicine and The
作者:Xu Rongxiang 出版社:CHINA SOCIAL SCIENCES PRESS 发行日期:2009 SeptemberDespite continuous progresses in science and technology, few attempts have been made to successfully develop functional tissue or organs from human cells. The exception is our embryology study and our work on the adult stem cells in vivo and in situ. Almost one decade ago, American researchers tried to establish a new life science system using various approaches and electronic technologies, but ended up only describing an ideal blueprint for the human genome. However, without sufficient understanding about cells, the genomic research that only focuses on life substance within the cell is of little applicable value since genes play their roles under the assistance of the function of cells. It is true that genomic research is very important in the life science, but such research will accomplish nothing if it is removed from cellular biochemistry and cytology. While an important approach to life science research, gene technology proves inadequate to solve any health problem or cure any disease unless combined with appropriate use of cytology focused on harnessing the function of the cell, life’s smallest unit.
Stem cell research and its application is another hot topic in life science apart from genomic. According to current reports from over the world, the most advanced stem cell research is the isolation and culture of stem cell in vitro before transplanting “tissue” which has been engineered (example: epithelium tissues and cartilage transplanted into the patients). However, a challenging problem that remains unsolved is how to maintain continuous proliferation of stem cells in vitro. It is well known that the environment in vitro does not completely meet the actual physiological requirements as that in vivo and in situ. The inadequate transmission of information and suboptimal regulation between histiocytes tissue cells results in an inadequate physiological linkage and constitution. This failing is magnified when the scale increases to commensurate with the macro-physiological function of tissue or human organs. Our research focused on the adult stem cells* in vivo and in situ and revealed that the damaged tissues and organs are able to repair themselves only if the adult cells can be transformed into stem cells with the potential of reconstituting tissue and organs. Until now, we have accomplished physiological tissue repair and functional organ regeneration in situ by cultivating skin stem cells in deep burn management. The following is the briefing of our current research status and achievements.
*Adult stem cell: Now we named these special cells “potential regenerative cells”(PRCs), which means that the special differentiated histiocyte tissue cell has the potential ability to regenerate to a functional tissue similar to a stem cell but normally exists in tissue as a histiocytetissue cell. It can also be called the special differentiated histiocyte tissue cell in all types of organs in the organism coming from proliferating cells during different development stages.
The major difference between PRC and adult stem cell (SC) is: PRC is a mature differentiated tissue cell, while SC normally refers to the undifferentiated cell. Some SCs can be identified by some special markers and, in skin regeneration, SCs are the proliferating form of PRCs. SCs can repair injured and defective skin by restructuring and regenerating new skin according to the original skin physiological structure.
1. Gastrointestinal Mucosa Regeneration
One paper published in Science in December 7, 2001 issue evoked great responses in the field of cell and tissue research. The authors collected small intestine tissues from embryonic mice and identified the types of cells by a special staining approach. The tissue slices from 17-day-old mouse embryo showed that the intestinal epithelium derived from four principal cell types. The report is an experimental study describing in detail that intestinal mucosa villas are composed of many types of cells.
We herein compared their reports to our results in cloning villas of small intestine with cells. We cultured gastric and intestinal wall tissue from mouse embryos in vitro, using a tissue culture composition called GIC that can promote the proliferation of stem cells*. The results showed that in the culture of gastric tissues, GIC stimulated the cells cluster beneath the gastric wall mucosa to persist in division and to form new tissue by proliferation. In the culture of intestinal tissues, GIC initiated the cells adjacent to the intestinal wall mucosa to become the stem cells with potential of proliferation. They ultimately differentiated into brush_border muscosa with absorptive function, or into endocrine cells in intestinal tract that proliferated until forming new intestinal tissues. The intestinal tissue section worked upon by American researchers is identical to our cultured intestinal tissue section. As a thought for a further step forward, we have reliable results in many functional assays. The cloning process of our gastrointestinal tissues in vitro can be visible during the months of culture but this itself is only attainable through the development of stem cells.
This is the first time in the history of life sciences that tissue or organs can develop in vitro. To ensure the novelty of our achievement, we have conducted a worldwide search of the published literatures on this subject. The search by a subsidiary of the National Science and Technology Ministry did not reveal any report of similar results. The website of www.stemcellresearchnews.com in the United States covered our results as the headline news on the issue of December 23, 2001.
These results offer proof that we have successfully cloned two different types of organs, stomach and intestine in vitro. GIC, as the necessary substance for cells, serves as the nutritive culture medium and protector. It is regarded as the only agent currently available for initiating cells to proliferate in order to repair tissue. The research of the role on GIC in promoting the growth of mucosal stem cells in the gastrointestinal tract (GI tract) has great clinical value. In the treatment of gastric diseases, GIC can protect the gastric wall and also repair ulcerative tissues. GIC can repair injured intestinal mucosa, and ensure intestinal mucosal cells’ ability to absorb nutriments. Using a mouse model featuring acute mucosal ulcers, we found that a 3-day treatment with GIC repaired the ulcers without scarring and resulted in recovery full function. GIC is suggested as the first priority before surgery for any gastrointestinal disease.
2. Nerve Regeneration
Sciatic nerves from white mice were sampled, cut in two and cultured in two different culture media in vitro with one containing GIC and the other with normal tissue culture medium without GIC. The results showed new nerve which had regenerated from the residual nerve cultured in GIC. Of note, the nerve in the control group shrank. Thus, we demonstrate that regenerative technology makes it possible to physiologically regenerate the defective nerve, thus advancing the tissue and organ regeneration from cytology to histology.
3. Kidney Regeneration
Failure of renal function is a very tough issue in medical practice. Because of pathological changes to the glomerulus and the renal tubules once deprived of filtering and reabsorption, a lot of patients need dialysis therapy. Our studies suggest a hope of regenerating glomerulus and renal tubules using regenerative technology. Cortical cells were taken from kidney and transformed to stem cells in culture. Glomerulus and renal tubules were formed by the cloning and constitution of stem cells. Regeneration in situ results are the same as the in vitro results, which begin when a regenerative substance is injected into a kidney with function failure. Animal experiments are now in process.
4. Marrow Regeneration
In this study, we took progenitor cells from marrow and cultured them in specific regenerative substances in vitro to form new marrow. Marrow transplantation is known as the best way to treat colony growth factors and the best method for promoting the formation of marrow progenitor cells. In our research, the regenerative potential of the progenitor was activated. One progenitor can develop into marrow consisting of various hematopoietic stem cells. The regeneration of human marrow tissue, once achieved in vivo and in situ, may lead to the possible cure of various blood disease.
5. Pancreas Regeneration
In histology and cytology, the function of the pancreas is as follows: The intestinal mucosa is stimulated by the food such as sugar or starch, then the intestinal mucosa sends the signal to the acinar cells to release amylopsin. After amylopsin enters into the intestine, the starch, after turning into glucose, is absorbed. Meanwhile, the acinar cell also informs its neighbor, the islet cell, to release insulin. At this point, the glucose is converted into energy by insulin after entering into blood. This whole process is controlled by endocrine and nerve functions. The two types of cell in the pancreas coexist and are codependent, each of them having its own secretory role.
Diabetes is the result of a disorder of growth and function of the acinar and islet cells of the pancreas. The disorder may result in excessive hyperplasia of the acinar cells (Type II diabetes) or atrophy of the islet cells (Type I diabetes). There is no physiologically effective therapy available to treat diabetes until now. It is necessary to understand how acinar cells grow and coexist with islet cells in terms of histological and cytological regulation. Some researchers only isolated and cultured islet cells from embryonic pancreas tissue in vitro, which destroyed the integrity of the pancreas. On the other hand, traditional Chinese medicine, working in conjunction with the laws of balance, suggests that both strengthening body resistance and consolidating the constitution are equally important therapeutic goals.
In the experiment, we found that all pancreas cells died after culturing in media only containing regular MEM media for 8 days. In contrast, in the other group, after coexisting for 65 days, acinar and islet cells established a harmonious proliferation when cultured in MEM medium containing additional “life substance”. On day 80, acinar and islet cells showed the tightest linkage until forming a new pancreas on day 92. Function examination on the nascent pancreas showed that before tissue necrosis in the control group, the amylopsin levels were remarkably different in the two groups. In the control group, it was several times higher than normal; but it was normal in the experimental group. Also, the pH value in the experimental group was normal while that in the control group was much higher. Determination of insulin showed that both the nascent and the mature pancreas is capable of producing abundant insulin while no insulin was produced in the control group because of the death of islet cells. These results indicated that normal pancreas tissue has been successfully cultured in vitro. Within 1 or 2 years, such results will be commercialized for therapeutic purposes and diabetic patients will be greatly relieved.
6. Skin regeneration.
Skin is the largest organ in human body. The commonly observed skin regeneration occurs as regeneration of epidermis, which is easily achieved as long as basal cells are available. In fact, skin regeneration is not as simple as the regeneration of cells, but involves the physiological adhesion, assembly and regeneration of multiple cells and multiple tissues with the final formation of functional full-thickness skin as a result. Full-thickness skin should include the combination of three germinal layers, physiological conjunction with subcutaneous tissues and coexistence with the host body. Therefore, it is inappropriate to define skin regeneration as the regeneration of any individual tissue or cell. Last year, in an international conference on stem cell research held in Singapore, French scientists, claiming to be “Father of Skin”, announced that they fulfilled skin regeneration in vitro. I questioned the French scientists whether the “skin” that they cultured was composed of epidermis, dermis and appendages, and whether the dermis further involved blood vessel, lymph, nerve, sebaceous gland, follicle and sweat gland. Therefore, a quotation mark should be added to their cultured “skin” as they, in fact, only cultured epidermis.
Skin histiocytes tissue cells are derived from three germinal layers: ectoderm, mesoderm and endoderm. Skin regeneration requires the regeneration of all skin tissue, such as muscle in endoderm, connective tissue in the mesoderm and epithelia in the ectoderm. Currently, we alone in the world of scientists have been able to accomplish the regeneration of skin. This book will cover our techniques in details and demonstrate how these techniques have been widely used in clinics as the dominant modality of burns therapy.
Surgical therapy has been the dominant approach in burns therapy all over the world for decades. However, almost all surgeons admit that they adopted surgical skin grafting not because it is the best therapy, but because quite simply it was the only choice. Surgery treats burns wounds by excising the burned skin and converts burns wounds into surgical wounds in preparation for skin grafting. This technique only treats complications of burns, instead of curing burn tissues. I was a surgeon for many years and I still remember when, as a student in medical school, teachers had such an expression that nobody would be willing to perform surgery as a burns treatment if skin regeneration were possible. Another instance, as textbooks indicate, second-degree burns healed below the scab by epithelial growth and covering the wound along the area below the scab, which indeed is the surgical way to heal the wound. Therefore, it is important to distinguish the two different medical conceptions.
As early as before 1989, we have matured burns skin regeneration therapy that was derived from successful burns treatment in clinic practice. Subsequent to burns, the human body has an instinct to initiate the regenerative potential of stem cells in vivo and in situ. However, the typical use of disinfectants and antibacterial agents on burns wounds makes it impossible to create a physiological environment sufficient to initiate and activate stem cell activation in burns wounds. The goal was to maintain and promote stem cells in order that they might proliferate and differentiate to further repair and clone organs.
In 1980s, I put forward an innovative conception on burn management, keeping the burn physiologically moist in order to promote repair and regeneration. This innovation finally led to the establishment of Burn Regenerative Medicine and Therapy (Moist-Exposed Burns Therapy, “MEBT”) and the discovery of Moist-Exposed Burn Ointment (MEBO), a topical drug used for maintaining a physiological environment for burns wounds. MEBO should be used under the technical criteria of burns regenerative therapy (MEBT) in order to fulfill the therapeutic potential. Years of clinical practice have testified that this treatment can heal deep second-degree burns without scarring and also to spontaneously heal superficial third-degree burns. Numerous successes of clinical practice encouraged me to further explore the mechanism of wound repair. Eight years of basic research disclosed that the mystery of physiological regeneration of burned skin lay in tissue stem cells. Based on this discovery, burns skin regenerative medicine was established and through the physiologically repairing and regenerating skin, we were able to culture of stem cells in vivo and in situ.
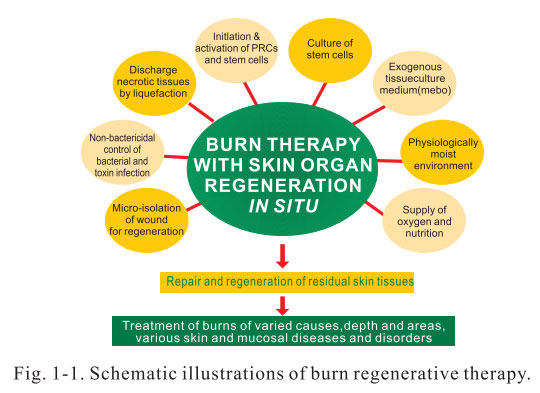
The principal part of BRT is MEBT and MEBO that consist of two procedures and eight techniques. Two procedures refer to liquefaction and discharge of necrotic tissues without causing secondary injuries, and maximum regeneration of skin tissue over the basal layer of viable tissue on wounds. Eight technologies include: initiation and regulation of stem cells; culture of stem cells in vivo and in situ; discharging necrotic tissues by liquefaction without causing further injury; exogenous tissue culture medium (MEBO) for skin regeneration; Physiological controlling bacteria and toxin infection by non-bactericidal mode; creation of a physiologically moist environment for skin regeneration; micro-isolation of skin wound for regeneration as well as supply of oxygen and nutriments required for skin regeneration (Figure 1-1).
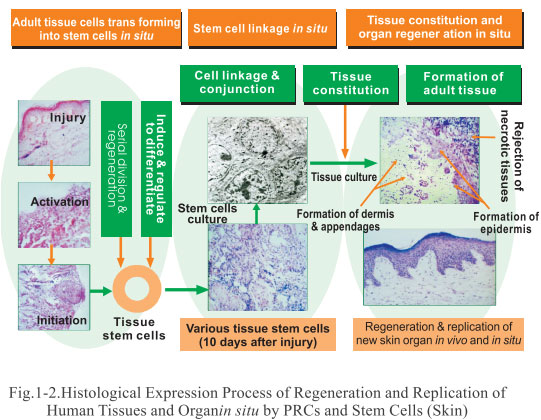
BRT is the only technology currently available to successfully repair and clone organs by the culture of stem cells in vivo and in situ. The cloning process of other organs will soon be identified subsequent to the success of cloning skin. On May 28th, 2002, we disclosed one of our research results “Mapping process of regenerating and cloning human tissues and organs” which has been submitted for patent application. The website www.stemcellresearchnews.com in the United States made a full coverage on this significant event. The mapping objectively demonstrated that evolvement of cells in repairing injured tissues is indeed a process of differentiation and integration. Firstly, when the body is injured, the viable cells in situ are initiated and transformed into adult stem cells. Secondly, adult stem cells are further induced and directionally differentiated into various tissue stem cells that will commit to tissue repair in the late stage. Thirdly, the nascent tissues come into being and the newly regenerated tissue stem cells further link with the nascent tissues. Finally, various nascent tissues integrate into the injured organ to form new functional tissue and organs and therefore fulfill the repair and regeneration of targeted tissues and organs in vivo and in situ (Figure 1-2).
This research result is a milestone in the human life science. It confirmed the assumption of the followings: 1) injured tissues have potentials to repair with full recovery of function in vivo and in situ; 2) activity of cells plays the principal role in this repairing process; and 3) it is within our ability to initiate the stem cells, regulate the directional differentiation, repair tissues and regenerate organs in vivo and in situ. which is only a small proportion of our scientific research results. Achievements on the repair and regeneration of other organs including stomach, intestine, marrow, pancreas, liver, kidney, heart as well as nerve will be published in separate volumes of Regenerative Medicine and Therapy. Regenerative Medicine, while a dream in the west, is happily a clinical reality in China. We are pleased to publishing volumes of Regenerative Medicine and Therapy in order to contribute to the knowledge base of scientists and doctors the world over who will be challenged and themselves stimulated by our advances in stem cell research. Notes: Comments from the publisher Dr.Xu-the inventor of MEBT and MEBO (moist-exposed burns ointment) gives an in-depth description of how healthy and pathological tissues behave in varied treatments environments. Further, he demonstrates that ordinary cells can differentiate into varied organ tissue and, for the first time, introduces MEBT including the use of MEBO to the western scientific community. This publication will add a new dimension to the discussions on stem cells, burns treatment, immunology and cell biology. Burns specialist will learn of the new gold standard in burns treatment, and cell biologists of the potential of ordinary cells.
The mapping process of regeneration and duplication of human tissues and organs in vivo and in situ represents a general and typical process. While each different tissue or organ has its own mapping, we will publish them shortly. Figure 1-3 shows the histological expression process of regeneration and duplication of human skin tissue and organs in vivo and in situ by adult stem cells after burns.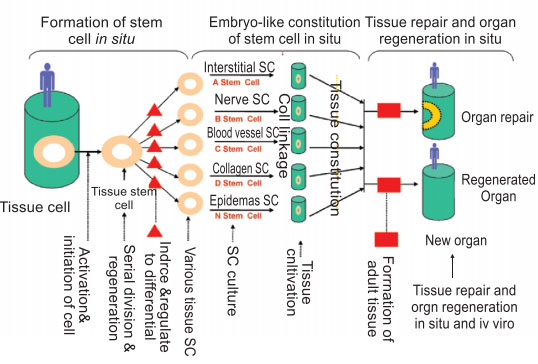
Above, we present the basic concept of regenerative medicine. Future research in this field requires deliberative and cooperative efforts between scientists and doctors from every country. Embryonic stem cell research is one of the approaches, but it has little value of clinical application as the tissue and organs of human are more appropriately and advantageously considered as a whole system. Available successful clinical results from traditional Chinese medicine should be considered as the basis of regenerative medicine research in “total” practice. Traditional Chinese medicine offers a valuable philosophy that should be further expanded through the incorporation of concrete scientific methodology, innovative research approaches, well-established scientific thoughts, rational analysis and rigorous conclusion. This is our common course as we establish a systemic academic college of world-class scientists. We believe that significant achievements in regenerative research will be ultimately obtained through our collaborative efforts and we welcome all who in a like manner will apply themselves to this noble cause.
1. KARGER publisher with a history of more than 100 years is one of the four greatest biomedical publishers in the world, together with McGraw-Hill, Mosby, John Wiley&Sons, and Oxford. As an internationally famous publisher, KARGER owns worldwide branch offices and distribution centers. At present, according to its medical model transformation, KARGER has taken timely steps to do researches on book markets and target readers. More over, its strict and professional proofreading procedures have ensured the high quality, high-level materials, high scientific value, international powerful influence and authority of all the publications. Burns Regenerative Medicine and Therapy is the first English monograph in the world on systematical introduction of regenerative medicine and therapy; the first monograph on the theory of regenerative medicine in situ and successful clinical practices; the first monograph on the field written by a Chinese; the first monograph published by the internationally famous publisher
2. Comments on Burns Regenerative Medicine and Therapy by KARGER
KARGER is one of the biggest and most famous medical and biological publishers in western world. All the famous medical monographs written by western scientists are published by it. The comment from the publisher on the book is revolutionary and amazing!
"Regenerative Medicine" is an innovative concept representing a unique approach to the regeneration of functional tissues and organs. This book reveals the scientific principles behind this newly discovered practice while instructing the reader in the procedure of moist-exposed burns treatment (MEBT) and offering compelling examples of tissue and organ regeneration from ordinary cells incubated in potent nutrient baths.